

Colorado folks love to be out in nature, and nothing is better than being in nature on a mountain bike. You can cover a tremendous amount of ground and see much more of our beautiful state on a mountain bike.
Unfortunately, just like everything else that is fun, there are dangers that you always are trying to avoid. Lose your focus for one split second, and you go down. Most of the time, you get up, brush yourself off and get back at it. But occasionally, your fall is not so smooth, and you land directly on one shoulder. The result – a clavicle fracture.
Clavicle fractures are relatively common and account for 5% of all fractures. A very high percentage of these fractures occur when falling directly onto the shoulder with all of your body weight. Here in Colorado, a majority of the clavicle fractures that I see are the result of mountain bike crashes. And #CaptainJacks is the “Usual Suspect.”
The clavicle is a very important bone as it connects our entire arm to our skeleton. The only attachment of our index finger to our skeleton is through the sternoclavicular joint. If the clavicle is fractured, it can disrupt the entire balance of that arm. Historically, the vast majority of these fractures have been treated without surgery. “Simply wear a sling, and it will heal fine.”
Unfortunately, this old-school thinking is dead wrong. A study that was performed by the Canadian Orthopaedic Trauma Society and published in the Journal of Bone and Joint Surgery in 2007 completely changed the narrative on clavicle fractures. They demonstrated that the outcomes with non-operative treatment were not as good as once thought. The failure to heal percentage in the operatively treated group was only 3%, while the non-operative group was 14%. The time to heal was 28 weeks in the non-operative group vs. 16 weeks in the surgical patients. Further, the patients in the non-surgical group had an overall complication rate of 63% vs. 37% for the surgical patients. And lastly, fracture displacement and clavicle shortening (due to overlap of fragments) are significantly associated with poor outcomes. Overlapping of the fragments > 15mm has subsequently been shown to significantly affect shoulder girdle strength due to the shortening of the muscle tendon units.
Thus, many of the clavicle fractures that have been traditionally treated conservatively with a simple sling, shoulder immobilizer, or clavicle strap are now treated with surgical repair. There are two methods for surgical treatment of clavicle fractures, plate fixation or intramedullary fixation, and each has its place depending on fracture configuration and degree of comminution (how many fragments are involved).
Intramedullary Fixation
Intramedullary fixation of clavicle fractures involves repairing the fracture with a rod inserted inside the intramedullary canal of the clavicle and crossing the fracture. It has some distinct advantages over plate fixation. First, the procedure can be performed through very small incisions, so it is much less invasive than plate fixation. Second, the IM rod can be easily removed after the fracture has healed. This technique is only applicable to fractures that have minimal comminution (not a lot of fragments), and there are not many surgeons that are familiar with this technique.
A well-known shoulder surgeon, Carl Basmania, pioneered this technique when he was responsible for taking care of Airborne Army Soldiers. He found that these soldiers were unable to continue with their duties after plate fixation because the plates were prominent over the surface of the clavicle and prevented them from being able to wear their rucksacks (80-pound backpacks). The plates caused pain where the shoulder strap hung over their clavicle. We are not able to remove these plates until complete fracture healing, which is typically not until 9-12 months after surgery. By the time this happened, many of these soldiers were discharged from service because they were not able to continue their duties. Conversely, those that underwent IM fixation were able to return to full duty by 8-12 weeks after surgery, and the rod was removed around 12 weeks after surgery.
I was lucky to train with Dr. Basmania and learn the idiosyncrasies of this technique and when it is applicable.
Case Example of IM Fixation

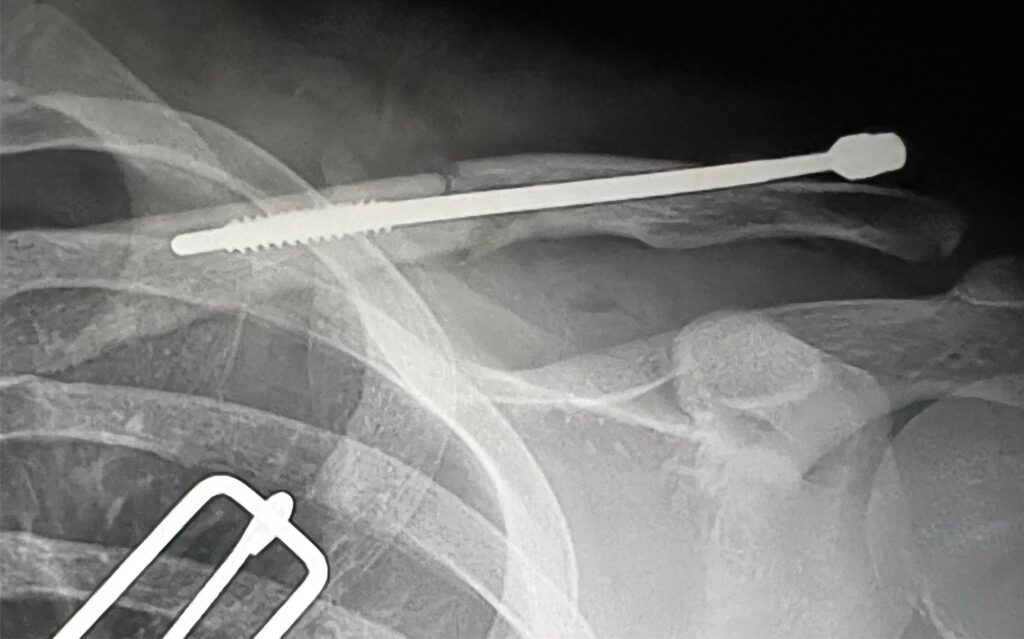

This is a 21-year-old male that had a mountain bike crash and fell directly onto his shoulder. He suffered a mid shaft clavicle fracture without significant comminution, but the fracture resulted in the shortening of his clavicle by over 2cm. He underwent IM fixation of his clavicle fracture utilizing the Rockwood Clavicle IM Rod. The rod was subsequently removed at 10 weeks post-op after adequate healing had occurred.
Case Example of Plate Fixation
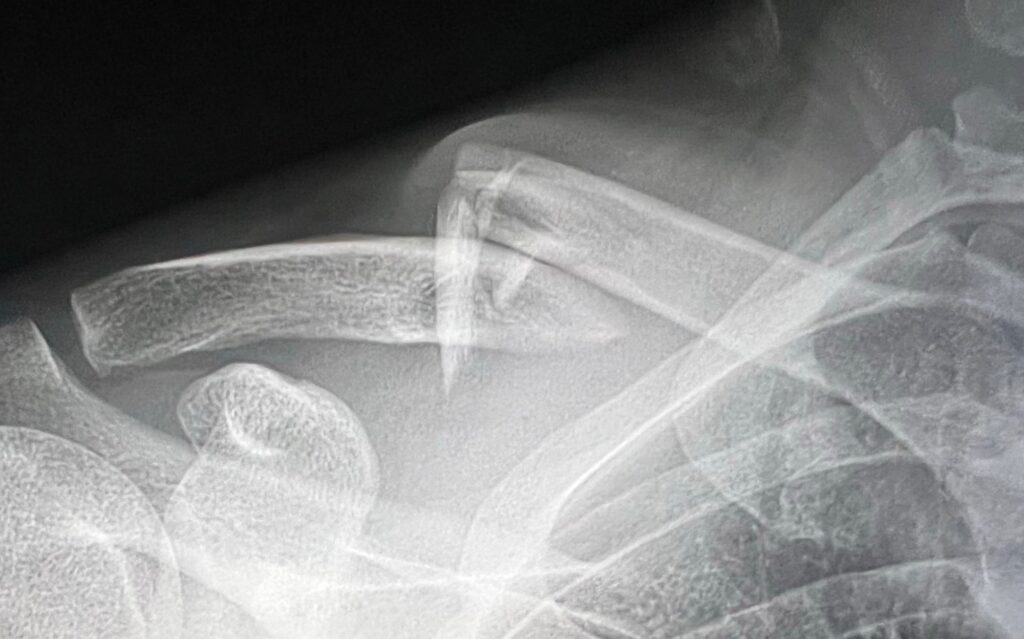
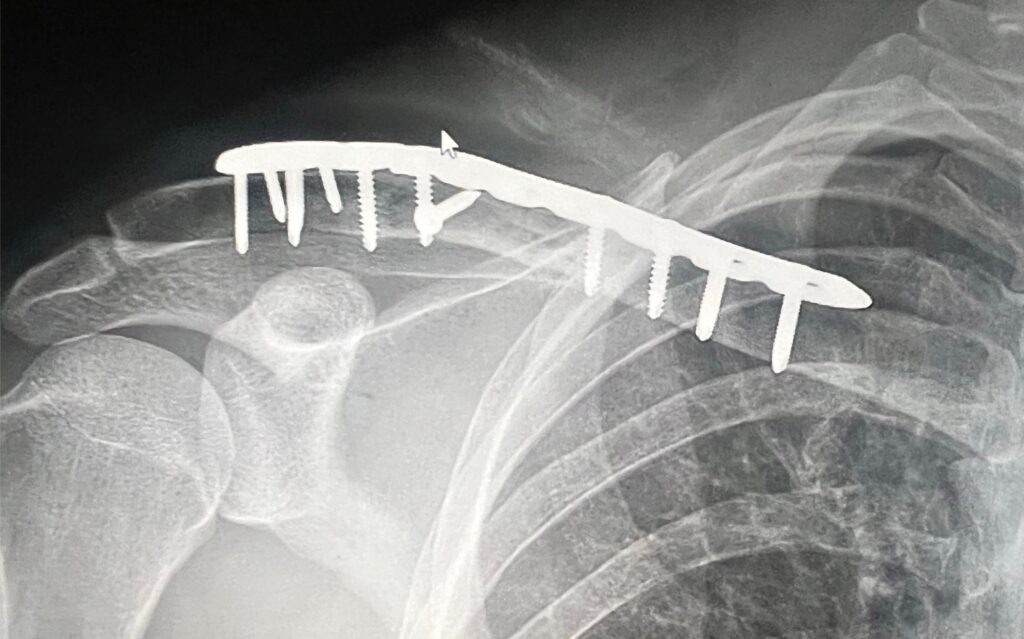
31-year-old male who suffered a very comminuted fracture of his clavicle after a mountain bike crash where he landed directly on his shoulder. His X-rays and surgical findings demonstrated severe comminution over a 3 cm segment of his clavicle. Due to the severe comminution, plate fixation was chosen.
The best treatment for each individual clavicle fracture will be determined by your treating surgeon. In order to receive the best treatment possible, you should seek the advice of a surgeon who is knowledgeable in the most advanced surgical options.



