

Rotator Cuff Tears
Rotator Cuff Tears – What You Need to Know
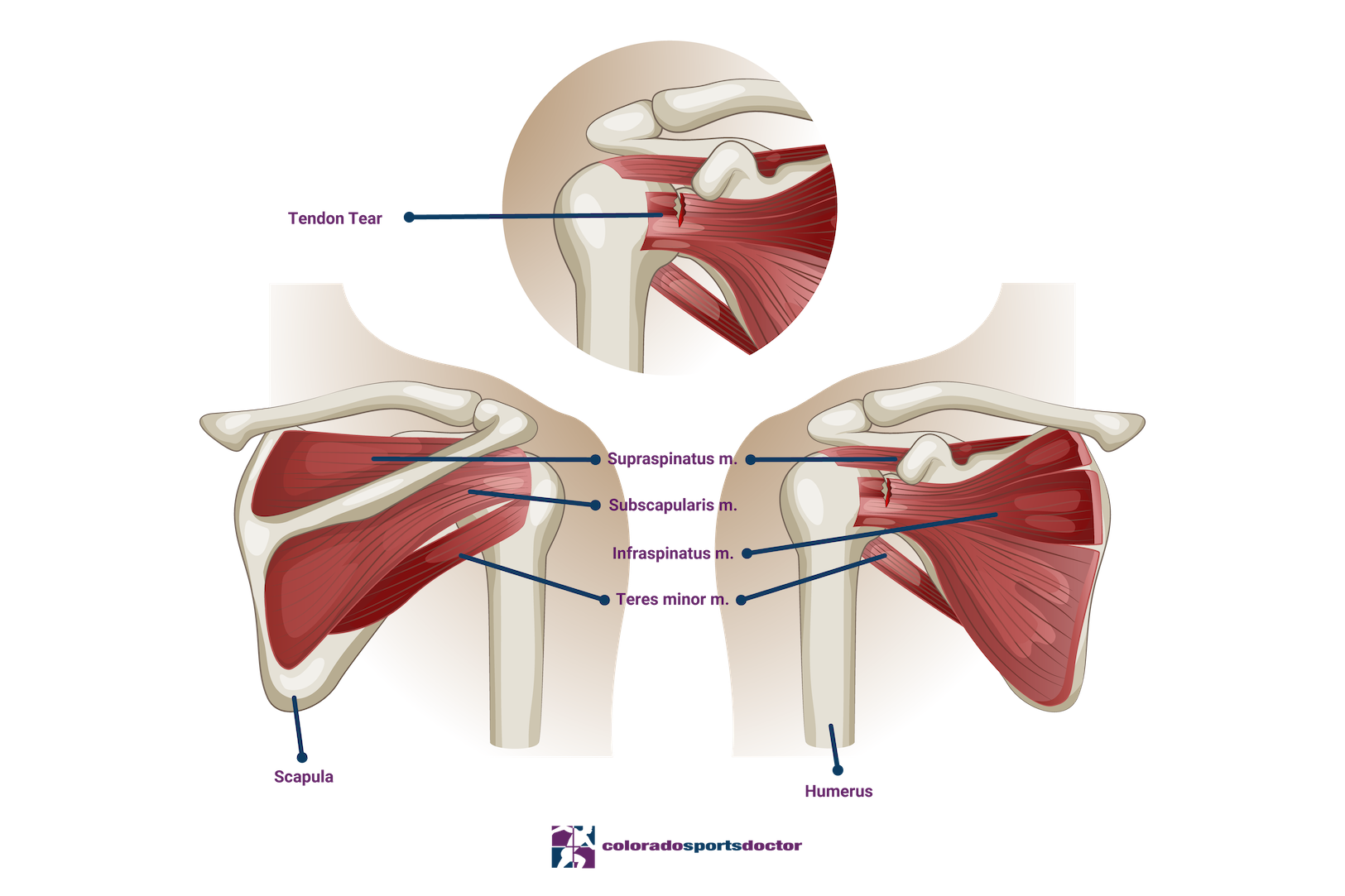
The rotator cuff is a commonly injured group of muscles that can experience different degrees of strain and tearing. The supraspinatus muscle stabilizes and lifts the arm, the infraspinatus rotates the arm outward, the teres minor also assists in external rotation and helps stabilize the shoulder joint, and the subscapularis muscle aids in the internal rotation of the shoulder.
The biceps tendon attaches to the top of the glenoid and passes through the rotator cuff muscles. It stabilizes and supports the shoulder joint. Injuries may occur from age-related degeneration, overuse, or an acute traumatic event.
Rotator Cuff Tear Anatomy
Rotator cuff injuries can result from repetitive shoulder use, sudden trauma, or accidents such as a fall or sports injury. Tears are categorized as partial-thickness, which affects only part of the tendon, or full-thickness, which extends through the entire tendon.
Patients with a rotator cuff tear often experience pain, weakness, and a limited range of motion.
Treatments
Conservative treatment methods for rotator cuff tears include rest, anti-inflammatory medication, and physical therapy to regain strength and mobility. Corticosteroid injections may also help reduce pain in partial tears.
When non-surgical treatments do not provide relief, surgery may be required to repair the tear. Dr. Jones has extensive experience treating rotator cuff injuries and performs arthroscopic surgery using advanced techniques.
Calcific Tendonitis of Rotator Cuff
Calcific tendonitis occurs when calcium crystals build up within the soft tissues of the shoulder. Although the exact cause remains unclear, it most often appears in the shoulder and can also affect the wrist, elbow, knee, hip, or foot. This condition typically affects adults between 30 and 50 years old and occurs more frequently in women.
The calcium buildup may have a chalk- or paste-like texture and can trigger intense inflammation and pain. When a patient presents with shoulder pain rated 10/10 or visits the emergency department for unrelenting pain, Dr. Jones often considers calcific tendonitis as the first possible diagnosis. Because the deposit can take up space inside the tendon, it may cause impingement under the acromion of the shoulder.
Although calcific tendonitis often resolves on its own, the process can take years, so treatment is usually necessary.
Diagnosis for Calcific Tendonitis
To make a diagnosis, the doctor performs a physical examination and orders X-rays. The exam typically reveals limited shoulder motion and pain during specific tests. X-rays can show the calcium deposit within the rotator cuff. Ultrasound imaging also helps visualize the affected area.
Treatment for Calcific Tendonitis
Treatment usually begins with conservative measures such as pain medication and anti-inflammatory drugs like ibuprofen or naproxen.
Physical therapy focuses on restoring strength and shoulder function. Cortisone injections can further reduce inflammation and help control severe pain.
During ultrasound-guided barbotage, the physician numbs the area, pierces the lesion multiple times, and flushes it with anesthetic and cortisone. Some of the calcium crystals are removed with a syringe, and the remainder are gradually absorbed by the body.
When pain does not respond to these methods, Dr. Jones performs arthroscopic surgery. During the procedure, he opens the lesion and mechanically removes the crystals. In some cases, a rotator cuff repair is performed to close the defect left after the removal.
Recovery After Rotator Cuff Surgery
Recovery time depends on the severity of the injury and the type of surgery performed. After surgery, patients usually manage pain and swelling with medication and ice. Rehabilitation progresses through planned exercises and stretching over several weeks or months.
Regular physical therapy sessions help restore range of motion and rebuild strength in the shoulder. Following the recovery plan created by Dr. Jones is essential to prevent re-injury and support successful healing.
Pre-Operative Risks
Anesthetic Complications
Sore throat – During surgery, the anesthesiologist administers anesthesia through an endotracheal tube or a laryngeal mask airway (LMA). Most patients avoid this issue, but if it occurs, it usually resolves within 24 to 48 hours. Over-the-counter throat spray can provide comfort.
Nausea – Some patients experience nausea as a side effect of anesthetic medications. The anesthesia team takes preventive measures to minimize this risk. If you’ve had nausea during prior procedures, discuss it with the anesthesiologist beforehand.
Shortness of breath – Many shoulder surgery patients choose an interscalene block, which numbs the shoulder and arm. About 3 percent experience temporary shortness of breath from a nerve block that affects the diaphragm. This sensation fades once the block wears off, typically within 12 to 36 hours.
Surgical Risks and Complications
Bleeding – Excessive bleeding during shoulder surgery is rare. Dr. Jones notes that anti-inflammatory drugs or blood thinners can increase bleeding risk and impair visibility during arthroscopic procedures. Patients should stop these medications about a week before surgery, after consulting their prescribing physician.
Infection – Infections occur infrequently, estimated in less than 1 percent of shoulder surgeries. The most common issue is a small stitch abscess caused by the body reacting to dissolvable sutures. These usually resolve with a short antibiotic course. Deep infections are uncommon but may require additional surgery.
Nerve damage – This complication is extremely rare, particularly in arthroscopic shoulder surgery. If nerve irritation occurs, it almost always resolves with time.
Post-Operative Risks
Stiffness – A small percentage of patients develop frozen shoulder (adhesive capsulitis) following surgery. Excessive scar tissue limits shoulder mobility. Completing the rehabilitation program helps reduce this risk, and stiffness often improves naturally over time.
Failure of the repair – Even with proper surgical repair and rehabilitation, not all rotator cuff repairs fully heal. Larger or long-standing tears may have lower healing rates. In addition, re-injury or premature activity can disrupt recovery. Dr. Jones adjusts each post-operative plan based on the tear size and healing requirements.
Frequently Asked Questions
Your shoulder pain arises from a tear of your rotator cuff tendons. A tendon is a thick, cord-like structure that connects muscles to bones. The rotator cuff muscles arise from your scapula and connect to the greater tuberosity of your humerus.
The majority of rotator cuff tears are not the result of a single traumatic event, although symptoms can be initiated by such an event. These tears occur as the result of many small injuries that accumulate over time. There is an area in the rotator cuff referred to as “the watershed zone." In this zone, there is no blood flow and thus the healing capacity of the injured tendons is very limited. Therefore, these small injuries accumulate and result in a complete tear.
A bursa is a small sac of fluid that lies between the tendons and bones and serves to act as a cushion and allow the tendons to glide without friction. If this bursa is injured, it will become inflamed and create more fluid than normal. The pain results from the bursa being inflamed.
The long head of the biceps enters the shoulder between the 2 rotator cuff tendons in the front of your shoulder and attaches to the top of the glenoid (socket). It is exceptionally common for patients with a rotator cuff tear to also have damage to this tendon. This can be treated at the same time as your rotator cuff is repaired. It is typically repaired by relocating its attachment further down your arm. This eliminates it as a source of pain and completely preserves the biceps function.
Not all rotator cuffs require surgical repair. However, if it is causing pain and weakness that is not responding to conservative care, it is best to undergo a rotator cuff repair. At the same time, I can address other areas of pathology as well (biceps, bone spurs, labral tears, arthritis, etc.)
If your tear is not completely detached, you potentially could be a candidate for conservative care including physical therapy, activity modifications, steroid injections, or possibly even biologic treatments.
The surgery is done arthroscopically. An arthroscope is an instrument about the size of a pencil that has a camera on its tip that can be inserted into the joint in order to visualize the various structures. Three to five 5-8 mm incisions are made to allow me to insert instruments into the joint and repair the injured tissues. Typically, suture anchors are utilized to reattach the tendon to the bone.
The tendons are repairable in the vast majority of cases. In cases where the tendons are not repairable, I usually have some idea before surgery based on information from your preoperative examination and MRI. If this is the case, there are some other options for you. These include a simple debridement (clean up), superior capsule reconstruction, or reverse total shoulder arthroplasty.
Your pain will often improve with time, but the tear will not heal. Typically, the pain improves because you are modifying the way you do things and avoid stressing the shoulder. The vast majority of rotator cuff tears will get larger over time and can become irreparable as well.
This surgery typically takes between 1 and 2 hours and is done as an outpatient. Where your surgery is performed depends primarily on your insurance. My team will check into this and get all of the appropriate authorizations. You will go home the same day as your surgery.
This type of surgery is successful more than 90% of the time in terms of having significant improvement in your symptoms and return to functional activities. The smaller tears generally do better than the large and more chronic tears. A successful recovery will depend greatly on your following of post-operative instructions and participating fully in the rehabilitation process.
Surgery is a complex and delicate process designed to repair damaged structures deep within the human body. Complications can occur, but fortunately are rare. I have performed thousands of these procedures and take every precaution in order to avoid them. But even when all precautions are taken and the surgery is meticulously performed, they can still occur. Certain factors may slightly increase your potential risks such as previous surgeries on the same shoulder or coexisting medical conditions (ie. diabetes, heart or lung problems, cigarette smoking). The most common complications are outlined below.
You will be able to use your hand, wrist, and elbow at waist level as soon as you are comfortable after surgery. It is critical that you wear your sling for the entire 6 weeks following your surgery in order to protect the repair while it heals. You may remove your sling for physical therapy, showers, or if you are simply sitting. There will be no active motion of the shoulder during these 6 weeks. Your arm must remain at your side and you can simply move the elbow.
For most sedentary jobs, I recommend 3 to 7 days off work. All of your restrictions apply and you must wear your sling. For more physical jobs, you may return to light duty with no lifting, pushing, pulling, or carrying more than 1 or 2 pounds for 6 to 8 weeks. Your restriction will be increased to 5 to 10 pounds at 3 months with nothing overhead. Full release generally happens around 6 months.
Although you will do much of your rehabilitation at home, I strongly advise you to see one of our physical therapists on a regular basis throughout your recovery. They will help keep you on track by following my protocols and advising you on a home program.