

Anterior Cruciate Ligament (ACL) Tear
Anterior Cruciate Ligament (ACL) Tear
Visiting the doctor can feel stressful and emotional, especially when surgery might be necessary. The information below is designed to ease your concerns, answer key questions, and help you better understand what to expect.
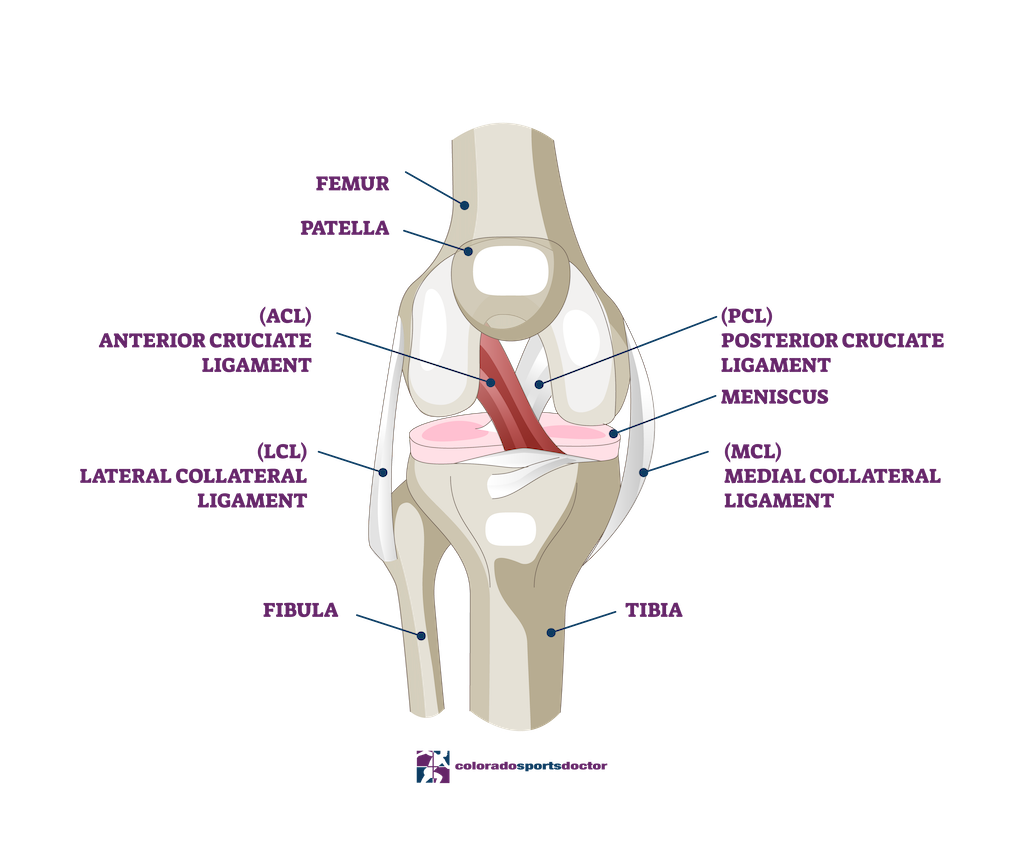
Knee Anatomy
The knee joint is a complex structure composed of bones, ligaments, cartilage, and menisci that work together to provide both stability and motion. The primary bones, the femur (thigh bone), tibia (shin bone), and patella (kneecap), meet at the knee joint. Ligaments such as the anterior cruciate ligament (ACL) connect these bones, preventing excessive movement and maintaining stability.
Cartilage is a smooth tissue that allows bones to glide over one another with minimal friction. The knee contains two types: articular cartilage, which covers the ends of bones, and meniscal cartilage, which consists of crescent-shaped discs that cushion and distribute weight.
When a ligament like the ACL tears, the knee’s stability is significantly reduced. The ACL is crucial for maintaining balance during cutting, pivoting, and running motions. Without it, the knee may buckle or give way, potentially leading to damage to the cartilage and menisci. Over time, this instability can increase the risk of developing osteoarthritis.
Injuries | ACL Tear
An ACL injury occurs when the ligament tears due to sudden twisting, rapid deceleration, or direct impact. As a result, the knee often feels unstable or gives way during movement. This injury is common among athletes and active individuals.
In many cases, other knee structures are also affected. The articular cartilage may fray, and the menisci can tear. These injuries often contribute to persistent pain and reduced joint function.
When the ACL is absent, the femur and tibia may slide incorrectly over one another, leading to additional wear on the joint. Over time, this mechanical stress can accelerate degeneration, increasing the likelihood of early-onset osteoarthritis.
Treatment & Recovery
Surgical reconstruction is often recommended for patients with a torn ACL, especially for those who wish to remain physically active. The goal of surgery is to restore knee stability and prevent further damage to cartilage and menisci.
During the procedure, Dr. Jones uses an arthroscopic-assisted technique, creating small incisions to access the joint. A new ligament, or graft, is constructed using tissue from the patient’s patellar tendon, hamstring tendons, or donor tissue. This graft is securely anchored to the bone to restore joint function. When damaged cartilage or menisci are identified, Dr. Jones repairs or trims them to promote smoother knee movement.
Recovery includes a structured rehabilitation program and gradual return to activity. Initially, patients use crutches and limit weight-bearing. With consistent physical therapy, they regain motion and strength over time. Most individuals return to routine daily activities within a few months, while returning to sports may take six to twelve months depending on progress.
Rehabilitation
Post-operative care focuses on reducing pain and inflammation while rebuilding strength. Many patients feel immediate relief after surgery because the knee is finally stable again. Early movement helps prevent stiffness and increases blood flow to the healing tissues.
Physical therapy plays a central role in recovery. For the first few months, patients usually attend therapy sessions multiple times a week to improve motion, build strength, and restore balance. Following the prescribed rehabilitation plan supports long-term success.
Most patients can resume sedentary work within a week. Those with jobs requiring standing or walking may need additional time. As strength improves, patients progress from using crutches to walking unassisted. For athletes or individuals in physically demanding jobs, the return to full activity requires extended rehabilitation to ensure proper healing and prevent re-injury.
Frequently Asked Questions
When you injured your knee, you tore one of the main ligaments which provides stability to the knee, the anterior cruciate ligament (ACL). Without the ACL, the knee will be unstable and give way if any side stepping, running or cutting motions are attempted. When your knee was injured, you may have damaged some of the cartilage and/or the menisci in the knee as well.
A ligament is a cord-like structure that connects two bones together at a joint and allows motion while providing stability. Stability refers to the joint moving in the proper plane while maintaining close apposition of the joint surfaces. When a ligament is torn, stability is compromised and the joint surfaces do not maintain this apposition and the bones can slide inappropriately on one another. This inappropriate motion can cause further damage to the cartilage and menisci.
Cartilage is the smooth white material that covers the ends of our bones in the joints. It provides a slick surface and allows the bones to glide over each other.
Menisci are another form of cartilage that look like bumpers between the bones. Their purpose is to provide cushion between the bones and disperse contact pressures over a greater area.
A physiologically young person who wishes to remain active will have a difficult time without a functioning anterior cruciate ligament. The knee will likely be unstable and suffer “giving way” or “buckling” episodes. During these episodes, the femur (thigh bone) and the tibia (leg bone) slide across each other and potentially cause new or further damage to the cartilage and menisci. For this reason, I recommend that you have surgery to correct the problem.
The goal of the surgery is to create a new ACL that will prevent the “giving way” or “buckling” episodes, and, hopefully prevent any further damage to the articular cartilage and menisci.
The ACL cannot be repaired because it is destroyed when it tears. Therefore, I make a new ACL using tissue that I take from somewhere else. This tissue can be from the patellar tendon in the front of your knee, your hamstring tendons, or allograft (donor) tissue.
Based on current medical knowledge, the likelihood of causing further damage to the knee and subsequently early onset of arthritis is very high.
Although brace construction has come a long way, the best brace cannot substitute for a functioning ACL. Studies indicate that braces may prevent instability episodes at low loads (walking), but at higher physiologic loads (cutting or pivoting) they cannot.
The surgery is done via arthroscopic-assisted technique. That means that although all of the work inside your joint is performed through three 1⁄2” incisions, the graft is harvested through an approximately 1 to 3 inch incision.
Yes, torn cartilage and menisci will either be debrided or repaired at the time of the surgery. Menisci are very important to the normal function of your knee so I am very aggressive in attempting to repair them if it is at all possible. If one of your menisci require repair, an additional 2-3 inch incision may be necessary on the inside or outside of your knee.
Depending on how much other damage is encountered in your knee, the surgery will take around two hours.
Patients enter the hospital in the morning, have surgery and go home the same day. This is called outpatient surgery.
This type of surgery is successful about 90-95% of the time. No operation is 100% successful in every patient, but the procedures we perform are reliable and will help restore your knee’s function. The success of your operation depends on many factors including:
- The amount of damage to the other structures in the knee
- Your body’s response to the injury and surgery
- Your compliance with post-operative rehabilitation
Surgery is a complex and delicate process designed to repair damage structures deep within the human body. Complications can occur, but fortunately are rare. Infection can occur (<1%) and may require antibiotics and surgery to clean out the joint. Injury to peripheral nerves can also occur but are also uncommon (<1%). Most often the injury is a stretch injury due to manipulation of the extremity during surgery or compression by the tourniquet. These are usually temporary and resolve by 2-6 weeks. Permanent injury can occur but is exceedingly rare. A small nerve that supplies sensation to the outside part of the leg just below the knee is almost always sacrificed during the graft harvesting. This may leave you with a small area of “numbness” on the front of your leg.
As soon as you are comfortable, I encourage you to be up and moving around. By the first or second post-operative day, I expect that you will move easily around your house with crutches and possible venture outdoors. As soon as you have recovered adequete quadriceps strength to support your weight without difficulty, I would like you to discard the crutches. There are particular circumstances where you will require a brace for a period of time, and I will let you know if that is the case.
For most sedentary jobs, I recommend a week off work. When you return to work your knee will be sore but you should be able to manage as long as you do no prolonged standing or walking. You will be on “light-duty” for 4 to 6 months depending on your work demands. These are merely guidelines and may need to be altered based on your individual recovery.
You can perform many of the necessary exercises by yourself at home. However, I ask that you work very closely with the physical therapist and plan on going to therapy 2-3 times per week for at least the first 2 or 3 months. After that time period your need for closely monitored PT will depend on your anticipated demand that you will place on the knee.