
Calcific tendonitis refers to a build-up of calcium crystals in soft tissues, and results in a “deposit” that is usually visible on a plain X-ray. The cause of this problem is not well understood, but is known to occur most commonly in the shoulder and is also seen in wrist, elbow, knee, hips and feet. This problem is typically seen in patients between the ages of 30-50 and is more common in women.
The calcium build up can have the consistency of chalk or toothpaste and can initiate a very bad inflammatory reaction in the involved joint. This will cause severe pain. When a patient presents with shoulder pain that is rated 10/10 or they have even been to the Emergency Department with intractable pain, Calcific Tendonitis is the first diagnosis that is considered. Further, the lesion can occupy more space than the normal tendon and can lead to impingement of the rotator cuff into the under surface of the acromial process of the shoulder.
The good news is that Calcific Tendonitis is typically self-limiting, meaning that it will eventually resolve on its own. The bad news is that it can take many years for this to happen. So patients will typically require treatment.
Diagnosis
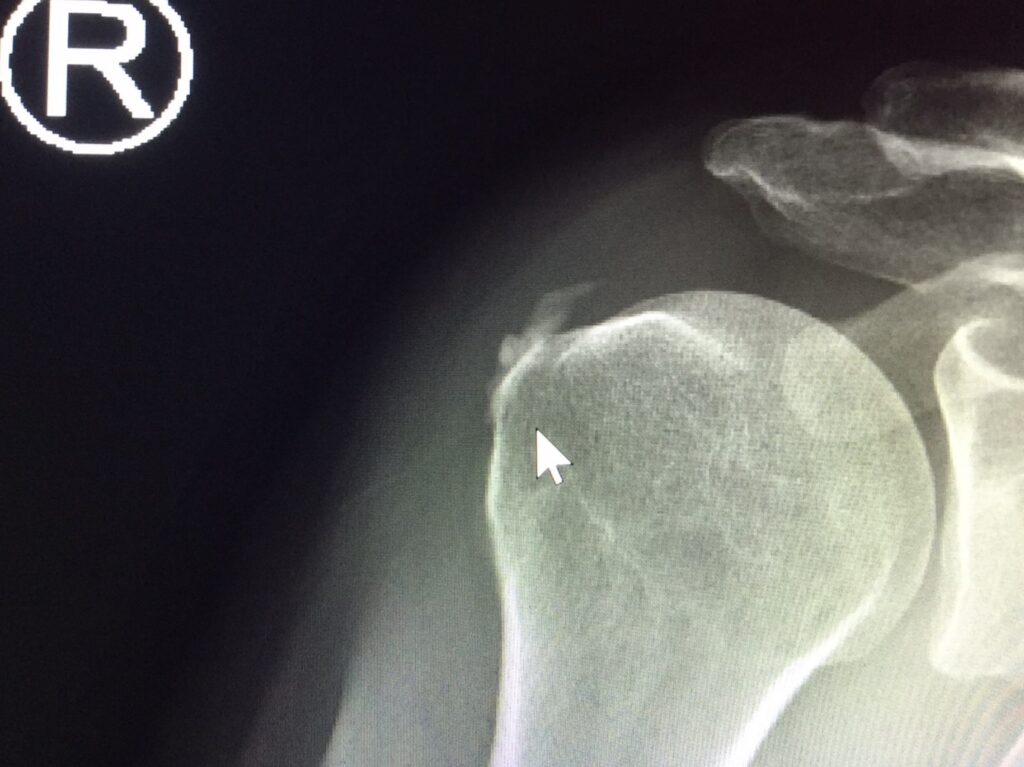
In order to diagnose this problem your doctor will typically perform a physical exam and get some X-rays. The examination will usually reveal some limitations of shoulder motion and significant pain on provocative test. X-rays will clearly demonstrate the calcium deposit within your rotator cuff.
Ultrasound is also very useful to visualize the deposit.

Treatment
Treatment of calcific tendonitis always starts with conservative measures which can include the following:
- Painkillers and anti-inflammatory medications (ie. Ibuprofen, Naproxyn)
- Physical Therapy – rotator cuff rehabilitation in order to restore strength and normal function of the shoulder.
- Cortisone steroid injections – reduces inflammation and is excellent at controlling the severe pain that this problem can cause.
- Ultrasound guided Barbotage – under ultrasound guidance the bursae is anesthetized with local anesthetic and the lesion is then pierced multiple times and “washed” with a combination of local anesthetic and cortisone. Some of the crystals are then aspirated out with the syringe. The remaining crystals are resorbed by the body.
- Surgical excision – Arthroscopic treatment is required only when the pain is not controlled with more conservative measures. During the arthroscopic treatment, the lesion is incised and the crystals are removed mechanically. Often this requires a rotator cuff repair be performed on the resulting defect in the rotator cuff.



